
The Evolving Landscape of Dementia Screening: Navigating Modern Cognitive Assessments for Early Detection and Proactive Care

Initial signs of cognitive decline—a mother forgetting a recent conversation, a spouse disoriented in a familiar grocery store—often trigger immediate concern and the daunting thought of dementia for caregivers. These moments of "brain fog" necessitate objective investigation, moving beyond anxious observation to informed action. Cognitive screening tests serve as a critical first step, transforming vague apprehension into a structured medical dialogue. While clinical terms like the Montreal Cognitive Assessment (MoCA) or the Mini-Mental Status Exam (MMSE) may seem intimidating, they are essential diagnostic tools, guiding families and healthcare providers through the complexities of aging and brain health. This article explores the evolution, efficacy, and future of these vital assessments, emphasizing their role in early detection, accurate diagnosis, and proactive care management.
The Imperative of Early Detection: Why Screening Matters
The global prevalence of dementia is staggering, with an estimated 55 million people living with the condition worldwide, a number projected to nearly double every 20 years, reaching 139 million by 2050. In the United States alone, over 6 million Americans are living with Alzheimer’s disease, the most common form of dementia, and this figure is expected to rise significantly. Beyond these statistics lie immense personal and societal costs, including diminished quality of life, emotional strain on families, and substantial healthcare expenditures. Early detection through cognitive screening is not merely about receiving a diagnosis; it is about unlocking a crucial window for intervention.
An early diagnosis of Mild Cognitive Impairment (MCI) or early-stage dementia allows individuals and their families to:
- Access Timely Treatments and Interventions: While there is no cure for most dementias, certain medications can help manage symptoms, and lifestyle interventions (diet, exercise, cognitive stimulation) can slow progression.
- Plan for the Future: Early knowledge enables crucial legal, financial, and care planning decisions to be made while the individual retains full capacity.
- Participate in Clinical Trials: Early-stage patients are often eligible for groundbreaking research studies, contributing to scientific advancement and potentially benefiting from new therapies.
- Mitigate Treatable Causes: As discussed later, many conditions mimicking dementia are reversible, making early screening vital for correct diagnosis and treatment.
Without effective screening, families often face delayed diagnoses, missing opportunities for proactive management and intervention, leading to greater challenges and distress down the line.
A Shifting Gold Standard: From MMSE to MoCA

For decades, the Mini-Mental Status Exam (MMSE), also known as the Folstein test, served as the primary cognitive screening tool in clinical settings. This 30-point questionnaire, taking 5-10 minutes to administer, assesses basic orientation, memory, attention, language, and visuospatial skills. While widely recognized and easy to administer, its limitations, particularly in detecting subtle cognitive changes, became increasingly apparent.
Modern clinical practice has largely shifted its preference to the Montreal Cognitive Assessment (MoCA). This 30-point test, developed in 2005 by Dr. Ziad Nasreddine in Montreal, takes 10-15 minutes and offers a more comprehensive evaluation of nine key cognitive domains: visuospatial/executive function, naming, memory, attention, language, abstraction, delayed recall, and orientation. The critical distinction lies in its sensitivity. Research, including a seminal 2005 study published in the Journal of the American Geriatrics Society, highlighted that the MMSE catches only about 18% of Mild Cognitive Impairment (MCI) cases. In stark contrast, the MoCA boasts a remarkable 90% to 100% sensitivity rate for detecting these early, subtle shifts that often precede full-blown dementia.
The MoCA’s superior ability to identify early impairment is largely attributed to its stronger emphasis on "executive function"—the brain’s "command center" responsibilities such as planning, problem-solving, organization, and mental flexibility. Tasks like abstraction (e.g., identifying similarities between a train and a bicycle), naming complex animals, and sustained attention tests are integral to the MoCA but less prominent in the MMSE. Relying on a less sensitive test like the MMSE can, therefore, create a dangerous "false sense of security," potentially delaying critical interventions. As medical professionals increasingly advocate, missing early signs is not merely a clerical error; it represents lost time that cannot be recovered.
Beyond the MoCA: A Spectrum of Screening Tools
While the MoCA has emerged as a frontrunner, several other cognitive screening tests serve specific purposes and clinical contexts:
- The Mini-Cog: A brief, simple test requiring only 3 minutes, ideal for primary care wellness exams. It combines a 3-word recall test with the Clock Drawing Test, providing a quick assessment of memory and visuospatial function.
- Self-Administered Gerocognitive Exam (SAGE): Developed by researchers at The Ohio State University, SAGE is a breakthrough for at-home health management. This 15-minute pen-and-paper test allows individuals to assess their cognitive health in a comfortable environment. Its unique design includes four versions to prevent the "practice effect" and an "Education Adjustment" for fairness across different educational backgrounds. Specific tasks include drawing a clock, naming items, performing calculations, and remembering words. The SAGE test empowers families to gather objective data before a doctor’s visit, transforming them from passive observers into proactive advocates.
- General Practitioner Assessment of Cognition (GPCOG): Tailored for primary care providers, the GPCOG includes a 4-minute patient assessment (testing time, orientation, clock drawing, recent event recall, word recall) and, if the score is indeterminate, an accompanying 2-minute informant interview with a caregiver to assess daily functioning and memory.
- Abbreviated Mental Test Score (AMTS): A quick, 10-item questionnaire assessing basic orientation and memory, often used in acute or emergency settings due to its rapid administration. Questions include age, current time/year, date of birth, and recalling an address.
- Memory Impairment Screen (MIS): A brief 4-item test specifically focused on memory impairment, involving a delayed-free and cued-recall test over about 4 minutes.
The "Imposter Factor": When Low Scores Aren’t Dementia
A critical understanding for caregivers and clinicians alike is that cognitive screens are precisely that—screens, not definitive diagnoses. A low score on any test, including the MoCA or AMTS (where a score of 6 or lower indicates impairment), does not automatically equate to an Alzheimer’s Disease diagnosis or any other form of dementia. These tests are designed to trigger further investigation, not to deliver a life sentence.

Numerous treatable "imposter" conditions can cause a patient to perform poorly on a cognitive screen, mimicking dementia symptoms. These include:
- Vitamin Deficiencies: Particularly B12 deficiency, which can lead to cognitive impairment, fatigue, and memory issues.
- Thyroid Disorders: Both hypothyroidism (underactive thyroid) and hyperthyroidism (overactive thyroid) can cause cognitive symptoms such as confusion, memory loss, and difficulty concentrating.
- Depression and Anxiety: Often referred to as "pseudodementia," severe depression can manifest with significant memory and cognitive deficits that improve with treatment of the underlying mood disorder.
- Urinary Tract Infections (UTIs): Especially in older adults, UTIs can cause acute confusion, delirium, and cognitive decline without typical urinary symptoms.
- Medication Side Effects: Polypharmacy (taking multiple medications) or interactions between drugs can lead to cognitive impairment, drowsiness, and confusion.
- Sleep Disorders: Conditions like sleep apnea can disrupt brain function and lead to daytime fatigue, poor concentration, and memory problems.
- Normal Pressure Hydrocephalus (NPH): A treatable condition involving an accumulation of cerebrospinal fluid in the brain, causing cognitive decline, gait disturbance, and urinary incontinence.
- Electrolyte Imbalances: Abnormal levels of sodium, potassium, or calcium can affect brain function.
- Dehydration: Can lead to confusion and cognitive impairment in older adults.
If a cognitive screening result indicates impairment, the next crucial step is a comprehensive medical evaluation. This typically includes a full blood panel (to check for deficiencies, thyroid issues, kidney/liver function), neuroimaging (such as an MRI or CT scan of the brain to rule out strokes, tumors, or NPH), and potentially a referral to a neurologist or neuropsychologist for a more in-depth assessment. This methodical approach ensures that reversible causes are identified and treated, preventing misdiagnosis and unnecessary distress.
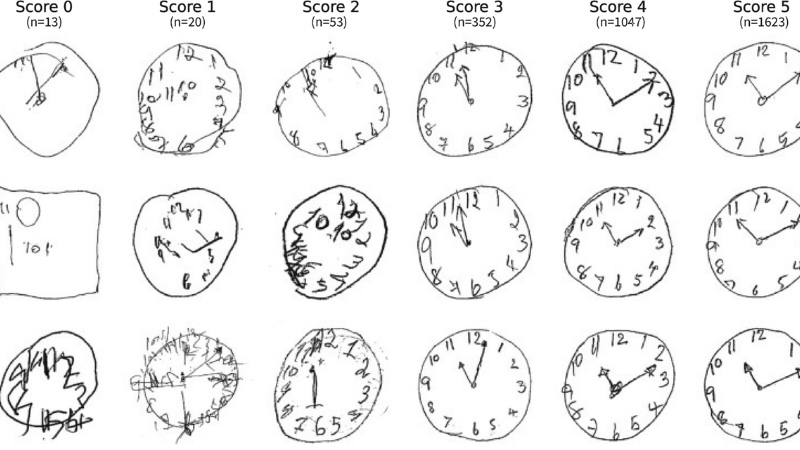
The Secret Language of the Clock Drawing Test
The "Clock Drawing Test" is a pervasive element across various cognitive screens, including the Mini-Cog, MoCA, and SAGE, for good reason. It is deceptively complex, offering a profound window into several critical cognitive domains. The patient is typically asked to draw a large clock face, place all the numbers, and set the hands to a specific time, often "10 minutes after 11."
This seemingly simple task demands a sophisticated interplay of cognitive functions:
- Visuospatial Abilities: The capacity to perceive and manipulate visual information, essential for drawing the circle and correctly spacing the numbers within it.
- Executive Function: Planning and organization are required to lay out the clock face logically.
- Attention: Sustained focus to complete the task accurately.
- Numerical Knowledge: Understanding the relationship between numbers and time.
- Abstract Reasoning: Translating a verbal command ("10 minutes after 11") into a concrete visual representation.
A person might exhibit near-perfect memory in other contexts but struggle significantly with the Clock Drawing Test—for instance, placing numbers outside the circle, omitting numbers, or incorrectly setting the hands. Such errors can signal stress on the brain’s visuospatial and executive communication pathways, often an early indicator of cognitive decline, even before more overt memory lapses occur. This makes the Clock Drawing Test a remarkably insightful and efficient component of cognitive screening.
Informant-Based Questionnaires: The Caregiver’s Perspective

In addition to direct patient testing, healthcare providers frequently utilize informant-based questionnaires, which leverage the unique observations of caregivers or family members. These tools are invaluable because patients, especially in the early stages of cognitive decline, may consciously or unconsciously minimize their difficulties, or genuinely lack awareness of their impairments. Caregivers, however, witness day-to-day functional changes that may go unnoticed in a clinical interview.
Key informant-based tools include:
- AD8 (Eight-item Informant Interview to Differentiate Aging from Dementia): This brief 8-question survey focuses on changes in functional abilities and cognitive skills over time. It asks about difficulties with judgment, hobbies, managing finances, remembering appointments, and daily tasks. A significant change reported by a caregiver can strongly indicate cognitive impairment.
- Short IQCODE (Informant Questionnaire on Cognitive Decline in the Elderly): This questionnaire asks a caregiver to compare the patient’s current cognitive abilities (e.g., memory for events, learning new things, handling money) to how they were 10 years ago. It helps quantify perceived decline.
These informant assessments are crucial for providing a holistic view of a patient’s cognitive health, capturing real-world functional changes that might not surface during a brief clinical examination.
The Digital Frontier: AI, Biomarkers, and Enhanced Precision
The landscape of dementia screening is rapidly evolving beyond traditional pen-and-paper tests, embracing digital innovation and advanced biological markers. As of 2026, many primary care offices are incorporating Digital Cognitive Assessments (DCAs). Platforms like BrainCheck and Cognivue offer several advantages:
- Standardization and Reduced Bias: Digital platforms eliminate human scoring bias, ensuring consistent administration and evaluation.
- Precision Tracking: They can detect and track subtle micro-changes in cognitive performance over time with greater accuracy than manual methods.
- Remote Monitoring: Some DCAs allow for remote administration, improving accessibility and continuity of care.
- Integration with Medical Records: Results can often be directly integrated into electronic health records, streamlining data management.
Beyond "thinking" tests, the rise of Digital Biomarkers is transforming early detection. These platforms use artificial intelligence (AI) to analyze subtle, often imperceptible, changes in a person’s voice, gait, eye movements, or even the way they draw a clock on a tablet. AI algorithms can identify "micro-hesitations" or patterns that the human eye or ear might miss, potentially signaling cognitive decline at ultra-early stages.
Perhaps one of the most significant advancements is the emergence of FDA-cleared blood tests for Alzheimer’s disease pathology. Blood-based biomarkers like pTau-181, pTau-217, and the Aβ42/40 ratio are revolutionizing the diagnostic pathway. These tests can accurately detect the presence of amyloid and tau pathologies—the hallmarks of Alzheimer’s—in the blood. For instance, the launch of pTau-181 blood tests for Alzheimer’s assessment in primary care represents a pivotal shift. A high-accuracy blood marker can help rule out Alzheimer’s pathology early, guiding primary care physicians on whether to refer a patient to a specialist for further, often more invasive, testing (like PET scans or cerebrospinal fluid analysis). This not only streamlines the diagnostic process but also reduces patient anxiety and healthcare costs.
Dementia Screening for Everyone: Culturally Fair and Specialized Tools
Standard cognitive tests, often developed in Western, English-speaking contexts, can sometimes be culturally biased or inappropriate for individuals with pre-existing intellectual disabilities or diverse linguistic backgrounds. To ensure equitable and accurate brain health assessments, clinicians are increasingly utilizing specialized tools:
- RUDAS (Rowland Universal Dementia Assessment Scale): Widely regarded as one of the most "culture-fair" tests, RUDAS is designed to minimize the influence of education, language, and cultural background. It uses tasks that are less dependent on formal schooling or specific cultural knowledge, making it suitable for multicultural populations and non-English speakers.
- NTG-EDSD (National Task Group Early Detection Screen for Dementia): This is the gold standard for screening dementia in adults with intellectual and developmental disabilities (IDD), such as Down Syndrome. Standard cognitive tests are often unsuitable for this population, as their baseline cognitive function may differ significantly. The NTG-EDSD considers these unique challenges, providing a more accurate assessment of cognitive change from an individual’s baseline.
These specialized tools underscore a growing recognition within the medical community that dementia screening must be inclusive and adaptable to diverse populations to truly serve everyone.
Conclusion: From Worry to Preparation and Proactive Management
The journey from initial concern about cognitive changes to a comprehensive understanding of brain health can be daunting for caregivers. However, the array of modern cognitive screening tests, from the highly sensitive MoCA to the at-home SAGE test and the cutting-edge digital biomarkers, provides powerful tools for navigating this path. The most important takeaway is that cognitive screening is fundamentally about preparation, not prediction. A "normal" score (e.g., 26-30 on the MoCA or above 6 on the AMTS) offers reassurance, while a score indicating impairment is not a final verdict but rather the beginning of a crucial diagnostic process.
Every screening result, whether indicating normal cognition or potential impairment, serves as a data point to inform the next chapter. It initiates a necessary conversation with a primary care physician, leading to a thorough medical panel including blood tests, neuroimaging, and potentially comprehensive neuropsychological testing to identify the true cause—be it a treatable "imposter" condition or an early stage of dementia. By choosing to screen for dementia early, caregivers are not merely seeking a diagnosis; they are taking a proactive, empowered role in managing their loved one’s brain health, laying the groundwork for informed decisions, timely interventions, and ultimately, a better quality of life. The evolving landscape of cognitive assessment offers unprecedented opportunities to shift from passive worry to prepared and proactive care.
Medical Disclaimer: The information provided in this article is for educational and informational purposes only and is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition or cognitive decline.




{kind=link}