
The State of Employer-Sponsored Health Insurance in 2025: Examining Access Disparities and Economic Barriers for the American Workforce
Employer-sponsored health insurance remains the primary pillar of the United States healthcare system, providing coverage to approximately 165.6 million people under the age of 65 as of March 2025. While this figure represents a significant portion of the non-elderly population, a comprehensive analysis from the Peterson-KFF Health System Tracker reveals that the distribution of this coverage is increasingly uneven, reflecting deep-seated economic divides within the American labor market. Despite the high aggregate number of insured individuals, the accessibility and affordability of workplace health benefits continue to vary drastically based on a worker’s income level, industry, and employment status.
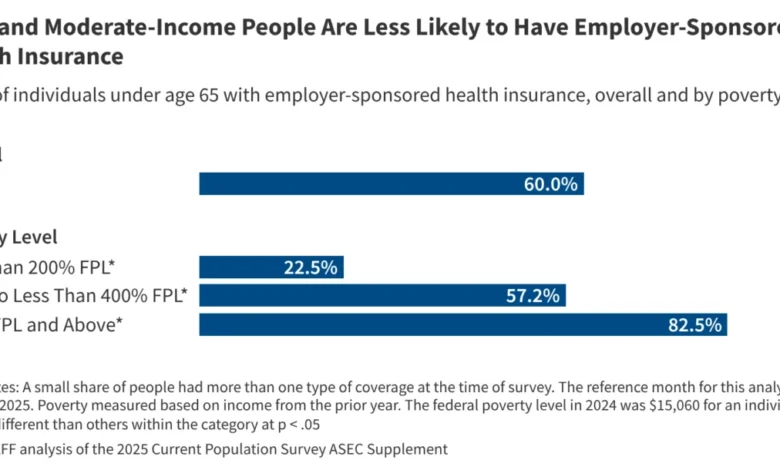
The most recent data, derived from the Annual Economic and Social Supplements of the Current Population Survey, underscores a persistent "coverage gap." While 80% of all adult workers under 65 are employed by companies that offer health insurance to at least a segment of their workforce, this availability drops precipitously to just 60% for lower-paid workers. This 20-percentage-point disparity highlights a structural challenge: the workers who are most vulnerable to high medical costs are often the least likely to be offered protection through their employers.
The Mechanics of Access: Offer Rates vs. Enrollment Trends
The disparity in employer-sponsored insurance (ESI) is not merely a matter of whether a company "offers" a plan; it is also a matter of eligibility and affordability. The Peterson-KFF analysis indicates that even when coverage is available, many workers remain uninsured or must seek alternative coverage through Medicaid or the Affordable Care Act (ACA) marketplaces.
For workers at the bottom of the income scale, the barriers are twofold. First, low-wage industries—such as retail, hospitality, and agriculture—are statistically less likely to provide comprehensive benefits compared to professional services or manufacturing. Second, even when low-wage employers do offer plans, the "take-up rate" (the percentage of workers who actually enroll) is significantly lower. This is often due to the high cost of employee-share premiums and high deductibles, which can consume a disproportionate share of a low-income worker’s take-home pay.
The data illustrates this income-based divide with startling clarity. Among people under 65 living in households with incomes at or above 400% of the federal poverty level (FPL), the ESI coverage rate stands at 82.5%. In contrast, for those with incomes below 200% of the poverty level, the coverage rate plunges to just 22.5%. This nearly four-fold difference suggests that for the American working poor, the promise of employer-linked healthcare remains largely unfulfilled.
A Chronological Context: The Evolution of ESI in the United States
To understand why the 2025 data reflects such significant disparities, it is necessary to examine the historical trajectory of employer-sponsored insurance in the U.S. Unlike many other developed nations that utilize centralized or single-payer systems, the U.S. model became tethered to employment through a series of mid-20th-century developments.
- The 1940s Labor Shortages: During World War II, the U.S. government-imposed wage freezes to prevent inflation. To attract workers without raising wages, companies began offering robust fringe benefits, including health insurance.
- The 1954 Tax Code: A pivotal moment occurred when the Internal Revenue Service codified the tax-exempt status of employer contributions to health insurance. This made ESI a highly tax-efficient way for employers to compensate employees, cementing the system’s dominance.
- The 2010 Affordable Care Act (ACA): The ACA introduced the "employer mandate," requiring businesses with 50 or more full-time equivalent employees to offer affordable coverage or face penalties. While this increased offer rates, it did not solve the issue of affordability for the lowest-earning employees.
- The Post-Pandemic Shift (2021–2024): Following the COVID-19 pandemic, a tightening labor market forced many employers to enhance benefits to retain talent. However, as the economy stabilized leading into 2025, inflationary pressures on medical costs began to outpace wage growth, leading some firms to shift a larger portion of premium costs onto employees.
By March 2025, the system reached the state observed in the Peterson-KFF report: a robust mechanism for the middle and upper classes, but a fragmented and often inaccessible one for those at the lower end of the economic spectrum.
Analyzing the 2025 Data: Supporting Statistics and Demographics
The 165.6 million people covered by ESI in 2025 represent a slight increase in raw numbers compared to previous decades, largely due to population growth and the continued strength of the labor market. However, the qualitative data reveals that the "quality" of this coverage is under pressure.
Industry experts point out that "underinsurance" is becoming as significant a hurdle as being "uninsured." Many low-to-moderate-income workers who fall into the 22.5% coverage bracket are enrolled in "Bronze-level" plans with deductibles exceeding $5,000. For a family living at 200% of the poverty level, such a deductible renders the insurance almost unusable for anything other than catastrophic events.
Furthermore, the eligibility criteria often exclude part-time workers. While 80% of workers are at firms that offer insurance, a significant subset of those workers—particularly in the "gig economy" or service sectors—do not work enough hours to qualify for those benefits. This "eligibility gap" is a primary reason why the 60% offer rate for low-paid workers does not translate into high enrollment.
Official Perspectives and Expert Reactions
Health policy analysts and economic researchers have expressed concern over the widening gap. While the Peterson-KFF Health System Tracker serves as an objective monitoring hub, the implications of its findings are frequently debated by stakeholders across the political and economic spectrum.
"The data confirms that employment is no longer a guaranteed ticket to health security in America," says one inferred analysis from health policy experts. "When we see such a massive discrepancy between high-income and low-income enrollment—82.5% versus 22.5%—it tells us that the current tax incentives and mandates are not reaching the people who need them most."
Labor advocates have reacted to these trends by calling for stricter definitions of "affordability" under federal law. Currently, an employer-sponsored plan is considered affordable if the employee’s contribution for self-only coverage does not exceed a certain percentage of their household income. However, advocates argue this formula fails to account for the cost of family coverage, which is often significantly higher, leading to the so-called "family glitch" that leaves dependents uninsured.
On the other side of the aisle, business groups often cite the rising cost of premiums as a barrier to expansion. With healthcare inflation frequently outstripping general inflation, small business owners in particular argue that they are being priced out of the benefits market, which explains why the offer rate for lower-paid workers (often employed by smaller firms) remains stuck at 60%.
Broader Implications for the U.S. Health System
The disparities in ESI coverage have far-reaching consequences for the broader U.S. healthcare infrastructure. When 165.6 million people are covered by private plans, the risk pool is substantial, which helps stabilize the market for the insured. However, the millions who are left out or priced out create a ripple effect.
First, the low enrollment among low-income workers puts increased pressure on public programs. Medicaid and the ACA marketplaces must "catch" those whom the employer-sponsored system drops. In states that have not expanded Medicaid, many of these workers fall into a "coverage gap" where they earn too much for Medicaid but not enough to afford their employer’s plan or a marketplace plan.
Second, the disparity exacerbates health inequities. Data consistently shows that individuals with employer-sponsored insurance have better access to preventative care, screenings, and chronic disease management. The low coverage rate (22.5%) for those under 200% of poverty directly correlates with higher rates of undiagnosed conditions and emergency room visits, which are the most expensive way to deliver care.
Finally, there is an economic implication regarding labor mobility. The phenomenon known as "job lock"—where workers stay in positions they dislike or are overqualified for simply to maintain health benefits—remains a factor in 2025. This limits economic dynamism and prevents workers from transitioning into entrepreneurial roles or smaller startups that may not offer the same level of benefits.
Future Outlook: The Path Toward Equity
As the Peterson-KFF Health System Tracker continues to monitor these trends, the conversation in Washington and state capitals is shifting toward how to bridge the 60% and 80% offer-rate divide. Potential policy interventions being discussed by researchers include:
- Enhanced Tax Credits for Small Businesses: Providing more aggressive incentives for small employers to offer plans to low-wage staff.
- Decoupling Coverage from Employment: Increasing the portability of health benefits so that coverage is not tied to a specific job, potentially through expanded HRA (Health Reimbursement Arrangement) models.
- Strengthening the ACA Employer Mandate: Lowering the threshold for "affordable" coverage to ensure that low-income workers are not forced to spend a crushing percentage of their income on premiums.
In conclusion, while employer-sponsored insurance remains the bedrock of American healthcare coverage in 2025, it is a bedrock with significant cracks. The 165.6 million people covered represent a success of the post-WWII economic model, but the 22.5% coverage rate for the working poor represents a systemic failure. As the year progresses, the data from the Current Population Survey will likely continue to serve as a catalyst for debates over how to ensure that the "employer-sponsored" label translates into actual health security for all segments of the American workforce.





{kind=link}