
White House Releases Fiscal Year 2027 Global Health Budget Request Proposing Significant Reductions and Program Restructuring
The administration officially submitted its Fiscal Year 2027 budget request to Congress on April 3, 2026, outlining a fiscal strategy that signals a pivot in the United States’ approach to international assistance and medical research. This comprehensive document details the proposed discretionary funding for global health programs managed by the Department of State, the Centers for Disease Control and Prevention (CDC), and the National Institutes of Health (NIH). Most notably, the request includes a series of significant reductions and a fundamental restructuring of the global health portfolio, moving away from long-standing funding levels to a leaner, more consolidated model.
The proposal arrives at a critical juncture in global health diplomacy. For decades, the United States has been the largest donor to global health initiatives, spearheading efforts to combat HIV/AIDS, tuberculosis, and malaria, while also bolstering maternal and child health services in low-income nations. However, the FY 2027 request suggests a departure from this historical trajectory. By proposing the elimination of specific programs and the tightening of discretionary spending, the administration is challenging Congress to reconsider the scope of America’s role as the primary financier of global public health.
The Department of State: Redefining Bilateral Assistance
Under the proposed FY 2027 budget, the Department of State faces some of the most visible structural changes. Historically, the State Department has overseen the President’s Emergency Plan for AIDS Relief (PEPFAR), one of the most successful public health programs in history. The new budget request, however, moves toward a "sustainability-focused" model that involves a reduction in direct bilateral funding.
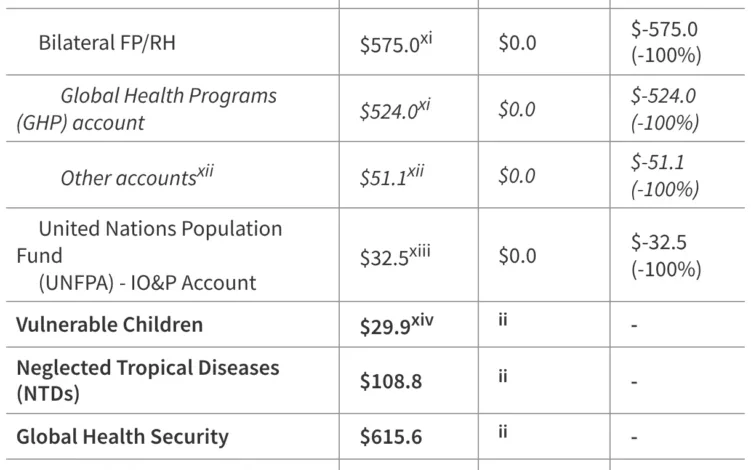
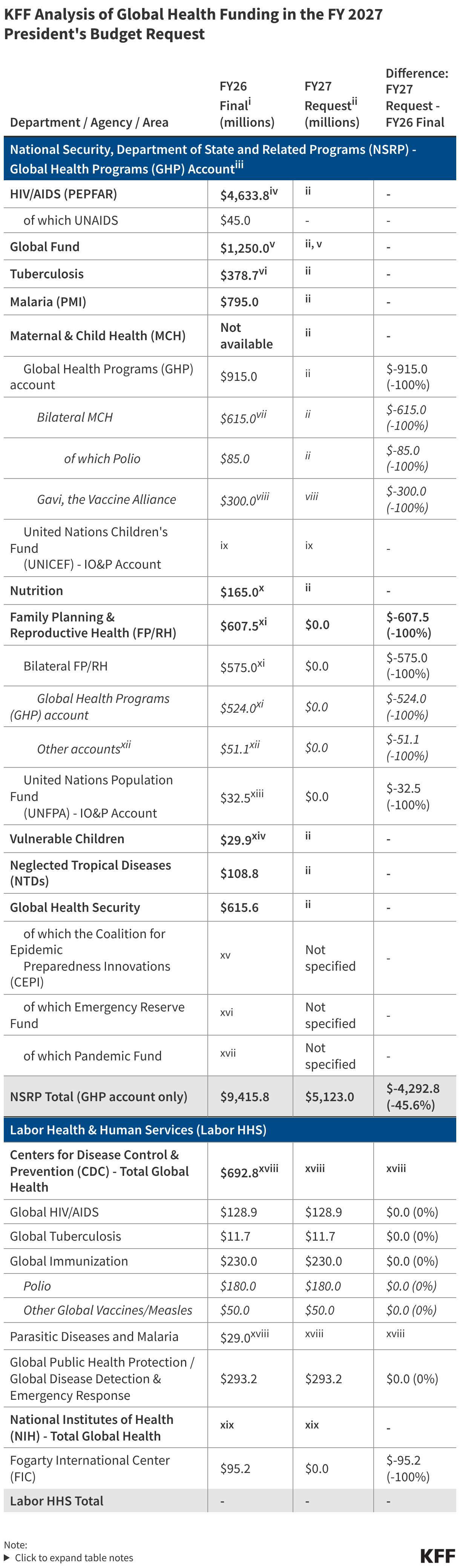
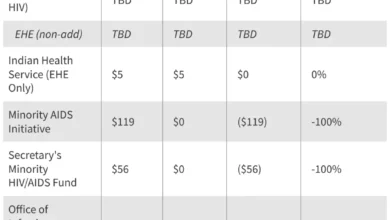
The administration’s request suggests a consolidation of several accounts within the Global Health Programs (GHP) window. While specific line items for HIV/AIDS, tuberculosis, and malaria remain, the proposed funding levels are notably lower than the enacted levels for FY 2026. Analysts from the Kaiser Family Foundation (KFF) note that the restructuring appears designed to transition more financial responsibility to partner governments. The budget request proposes the elimination of certain legacy programs that the administration deems have reached a stage where local ownership is feasible.
Furthermore, maternal and child health (MCH) funding, as well as voluntary contributions to international organizations, are slated for a downward adjustment. The administration argues that these cuts are necessary to balance the federal deficit while prioritizing "high-impact" interventions that offer the greatest return on investment in terms of lives saved per dollar spent. Critics, however, worry that these reductions could reverse gains made over the last twenty years in reducing child mortality and improving reproductive health access in sub-Saharan Africa and Southeast Asia.
Centers for Disease Control and Prevention: A Shift in Global Health Security
The CDC’s global health mandate has traditionally focused on technical assistance, disease surveillance, and the strengthening of laboratory systems worldwide. In the FY 2027 request, the administration proposes a restructuring of the CDC’s Center for Global Health. The budget emphasizes "Global Health Security" as the primary pillar, potentially at the expense of vertical disease programs like polio eradication and global immunization efforts.
The proposed budget includes a reduction in the CDC’s global tuberculosis and parasitic disease programs. By streamlining these activities, the administration intends to create a more "agile" response force capable of detecting emerging pandemic threats rather than maintaining permanent footprints for endemic disease control. This shift reflects a broader policy debate: whether the U.S. should continue to fund the eradication of specific diseases or focus exclusively on preventing the next global outbreak from reaching American shores.

Under the new plan, the CDC would see its global workforce footprint modified, with a greater emphasis on regional hubs rather than country-specific offices. This "regionalization" strategy is presented as a cost-saving measure, though public health experts warn it may diminish the agency’s ability to provide the granular, on-the-ground expertise that has been the hallmark of the CDC’s international reputation.
National Institutes of Health: The Future of Global Research
The National Institutes of Health, particularly the Fogarty International Center, has long been the engine of global health research and capacity building. The FY 2027 budget request proposes a tightening of the NIH’s discretionary budget for international collaborations.
A key area of concern for the research community is the proposed reduction in funding for the Fogarty International Center, which supports research and training for US and foreign investigators to work on health problems of global importance. The administration’s budget suggests that more of this research should be integrated into the broader domestic NIH institutes, potentially diluting the focus on neglected tropical diseases and health issues that primarily affect the Global South.
Additionally, the budget proposes a shift in how the NIH funds international clinical trials. The new directive prioritizes research with clear "dual-use" benefits—scientific breakthroughs that have immediate applications for the American healthcare system as well as global utility. While this aligns with a "taxpayer-first" research agenda, it may leave a vacuum in the study of diseases that do not pose a direct threat to the U.S. population but cause significant morbidity and mortality globally.
Chronology of the FY 2027 Budget Cycle
The release of the President’s budget request on April 3, 2026, marks only the beginning of a lengthy and often contentious legislative process. To understand the implications of this proposal, it is essential to look at the timeline ahead:
- April – May 2026: Congressional committees, specifically the House and Senate Appropriations Committees, will hold hearings. Cabinet secretaries and agency heads from the State Department, CDC, and NIH will be called to testify and defend the proposed cuts and restructuring.
- June – July 2026: The House and Senate will begin drafting their respective versions of the Labor, Health and Human Services, Education, and Related Agencies (Labor-HHS) bill and the National Security, Department of State, and Related Programs (NSRP) bill. Historically, Congress often restores funding that the administration proposes to cut, particularly for popular programs like PEPFAR.
- September 2026: This is the critical "markup" period where the final numbers are negotiated. If a consensus is not reached by September 30, the end of the fiscal year, a continuing resolution (CR) may be required to keep programs running at FY 2026 levels.
- October 1, 2026: The start of Fiscal Year 2027. Ideally, a finalized budget would be signed into law, but political polarization often delays this until late 2026 or early 2027.
Supporting Data and Comparative Analysis
When compared to the FY 2026 National Security and Labor-HHS conference bills, the FY 2027 request represents a proposed decrease in total global health spending by approximately 12% to 15%, depending on how "restructured" funds are categorized.
For example, the FY 2026 enacted budget for Global Health Programs at the State Department and USAID stood at approximately $10.5 billion. The FY 2027 request seeks to bring this figure closer to $9 billion. Within the CDC, the Global Health Security line item, which saw a surge during the mid-2020s, is proposed to be "stabilized," while other global health activities face cuts of up to 20%.
The NIH’s Fogarty International Center, which has traditionally operated on a modest budget of around $95 million to $100 million, would see its first significant nominal cut in over a decade under this proposal. These figures have sparked immediate concern among data analysts who track the correlation between U.S. funding and global health outcomes.
Official Responses and Stakeholder Reactions
The reaction to the April 3 announcement was swift. Global health advocacy groups, including the Global Health Council and the ONE Campaign, issued statements condemning the proposed cuts. "Slashing global health funding is not just a humanitarian failure; it is a strategic mistake," said a spokesperson for a leading international NGO. "U.S. leadership in global health is a cornerstone of our national security and diplomatic influence. Withdrawing now leaves a vacuum that other, less predictable global powers will be eager to fill."
On Capitol Hill, the reception was divided. Proponents of the budget within the administration’s party praised the "fiscal responsibility" of the request. "We cannot continue to spend at emergency-level rates indefinitely," noted one senior member of the House Appropriations Committee. "This budget reflects a necessary transition toward sustainable, partner-led health systems."
Conversely, a bipartisan group of lawmakers—many of whom have been long-time champions of PEPFAR—expressed skepticism. In a joint statement, several senators argued that the proposed "restructuring" could inadvertently dismantle the very delivery systems that allow the U.S. to respond to health crises efficiently. They vowed to work through the appropriations process to ensure that "life-saving programs remain fully funded."
Broader Impact and Strategic Implications
The implications of the FY 2027 budget request extend far beyond the balance sheets of federal agencies. If enacted as proposed, the restructuring of U.S. global health funding could signal a major shift in international relations.
First, there is the issue of "Soft Power." Global health has long been a "warm" entry point for U.S. diplomacy, allowing for cooperation even with nations where political tensions are high. By reducing its footprint, the U.S. may lose significant leverage and goodwill in developing regions.
Second, the "Pandemic Preparedness Gap" remains a concern. While the budget prioritizes Global Health Security, critics argue that security cannot be divorced from general health system strengthening. A country with a collapsed maternal health system or an unfunded tuberculosis program is unlikely to have the infrastructure necessary to detect or contain a new viral outbreak.
Finally, there is the "Human Cost." KFF’s budget tracker and historical analysis suggest that even minor fluctuations in funding can lead to gaps in service delivery. For HIV/AIDS patients, a transition to "local ownership" that is too rapid could lead to stockouts of antiretroviral drugs, potentially leading to increased viral resistance and higher mortality rates.
As the FY 2027 budget moves to the halls of Congress, the debate will likely center on a fundamental question: Is global health an elective charitable contribution, or is it an essential component of 21st-century American national security? The administration has made its opening move, proposing a leaner, more constrained vision. It is now up to the legislative branch to determine if that vision will become reality.





{kind=link}