
US Global Health Strategy and Bilateral Support Framework for Fiscal Year 2024 Mapping International Health Investments Across 80 Nations
The United States government has solidified its position as the largest donor to global health initiatives, maintaining a robust presence in more than 80 countries through bilateral programs and extending its reach even further via regional partnerships and multilateral organizations. As the world navigates the complexities of the post-pandemic era, the Fiscal Year (FY) 2024 data reveals a strategic focus on seven core pillars: the President’s Emergency Plan for AIDS Relief (PEPFAR), Tuberculosis (TB) control, the President’s Malaria Initiative (PMI), Family Planning and Reproductive Health (FP/RH), Maternal and Child Health (MCH), Nutrition, and the burgeoning field of Global Health Security. This comprehensive framework represents a multi-billion-dollar commitment aimed at stabilizing fragile health systems, eradicating infectious diseases, and fostering economic resilience through improved public health outcomes.
The Architecture of U.S. Global Health Engagement
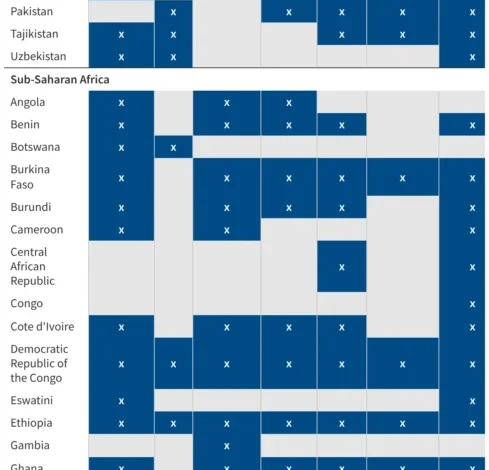
The U.S. bilateral global health portfolio is managed through a collaborative inter-agency approach involving the U.S. Agency for International Development (USAID), the Centers for Disease Control and Prevention (CDC), the Department of State, and the Department of Health and Human Services (HHS). Each partner country’s program is tailored to local epidemiological needs and national health priorities. In many regions, particularly in Sub-Saharan Africa and Southeast Asia, U.S. programs operate across multiple health areas simultaneously, creating a "braided" funding model that maximizes the impact of every dollar spent.
For FY 2024, the U.S. government has prioritized the integration of services. For instance, maternal health clinics are increasingly being used as entry points for nutrition counseling and malaria prevention. This holistic approach reflects a shift from disease-specific "silos" toward integrated primary healthcare strengthening. The current tracker data emphasizes that while some countries receive specialized support for a single threat—such as global health security in middle-income nations—others, termed "priority countries," receive a full suite of interventions across all seven programmatic areas.
A Chronology of Leadership and Evolution
The trajectory of U.S. involvement in global health has evolved significantly over the last six decades. While early efforts in the 1960s and 70s focused primarily on population control and basic immunization, the 21st century marked a paradigm shift toward massive, targeted interventions.
- 2003 – The Inception of PEPFAR: President George W. Bush launched PEPFAR, the largest commitment by any nation to address a single disease. Since then, the program has saved over 25 million lives and prevented millions of HIV infections.
- 2005 – The President’s Malaria Initiative (PMI): Following the success of PEPFAR, PMI was established to reduce malaria-related mortality by 50% across 15 high-burden countries in Africa.
- 2009 – The Global Health Initiative (GHI): The Obama administration introduced GHI to foster a more integrated approach, placing a heavier emphasis on maternal and child health and strengthening health systems rather than just treating diseases.
- 2014 – The Global Health Security Agenda (GHSA): Launched in response to emerging infectious threats, this initiative gained unprecedented momentum following the West African Ebola outbreak and, more recently, the COVID-19 pandemic.
- 2024 – Strategic Realignment: The current fiscal year focuses on "localization"—shifting the implementation of programs to local NGOs and governments to ensure long-term sustainability as U.S. funding fluctuates.
Deep Dive into Core Program Areas
PEPFAR and the Path to 2030
As PEPFAR enters its third decade, the FY 2024 strategy is focused on reaching the UNAIDS "95-95-95" targets: 95% of people living with HIV knowing their status, 95% of those diagnosed on antiretroviral therapy (ART), and 95% of those on ART achieving viral suppression. Data indicates that PEPFAR currently supports nearly 20 million people with life-saving treatment. The program is also increasingly focusing on the "DREAMS" partnership, which aims to reduce HIV incidence among adolescent girls and young women, who remain disproportionately affected in Sub-Saharan Africa.
The President’s Malaria Initiative (PMI)
In FY 2024, PMI continues to lead the global fight against malaria, a disease that still claims hundreds of thousands of lives annually, mostly children under five. The initiative focuses on the distribution of insecticide-treated bed nets (ITNs), indoor residual spraying, and the procurement of artemisinin-based combination therapies (ACTs). A significant development in the 2024 landscape is the rollout of the R21/Matrix-M malaria vaccine, which the U.S. is helping to integrate into routine immunization schedules in high-transmission areas.
Maternal, Child Health, and Nutrition
The U.S. remains a critical partner in reducing preventable maternal and child deaths. Bilateral programs in this sector focus on the "first 1,000 days"—from pregnancy to a child’s second birthday. Interventions include skilled birth attendance, newborn resuscitation, and the treatment of childhood pneumonia and diarrhea. In the nutrition sector, the U.S. is addressing the "double burden" of malnutrition—stunting and wasting—which has been exacerbated by global food insecurity and climate-related shocks.
Global Health Security: The New Frontier
Perhaps the most rapidly expanding area of the U.S. portfolio is Global Health Security (GHS). The FY 2024 data shows an increase in the number of countries receiving bilateral GHS support. The objective is to help nations comply with International Health Regulations (IHR) by improving laboratory networks, surveillance systems, and emergency operations centers. The goal is a "7-1-7" target: detecting an outbreak within seven days, reporting it within one day, and mounting an effective response within seven days.
Regional Distribution and Strategic Investments
The geographical distribution of U.S. global health programs reflects both humanitarian need and strategic interests.
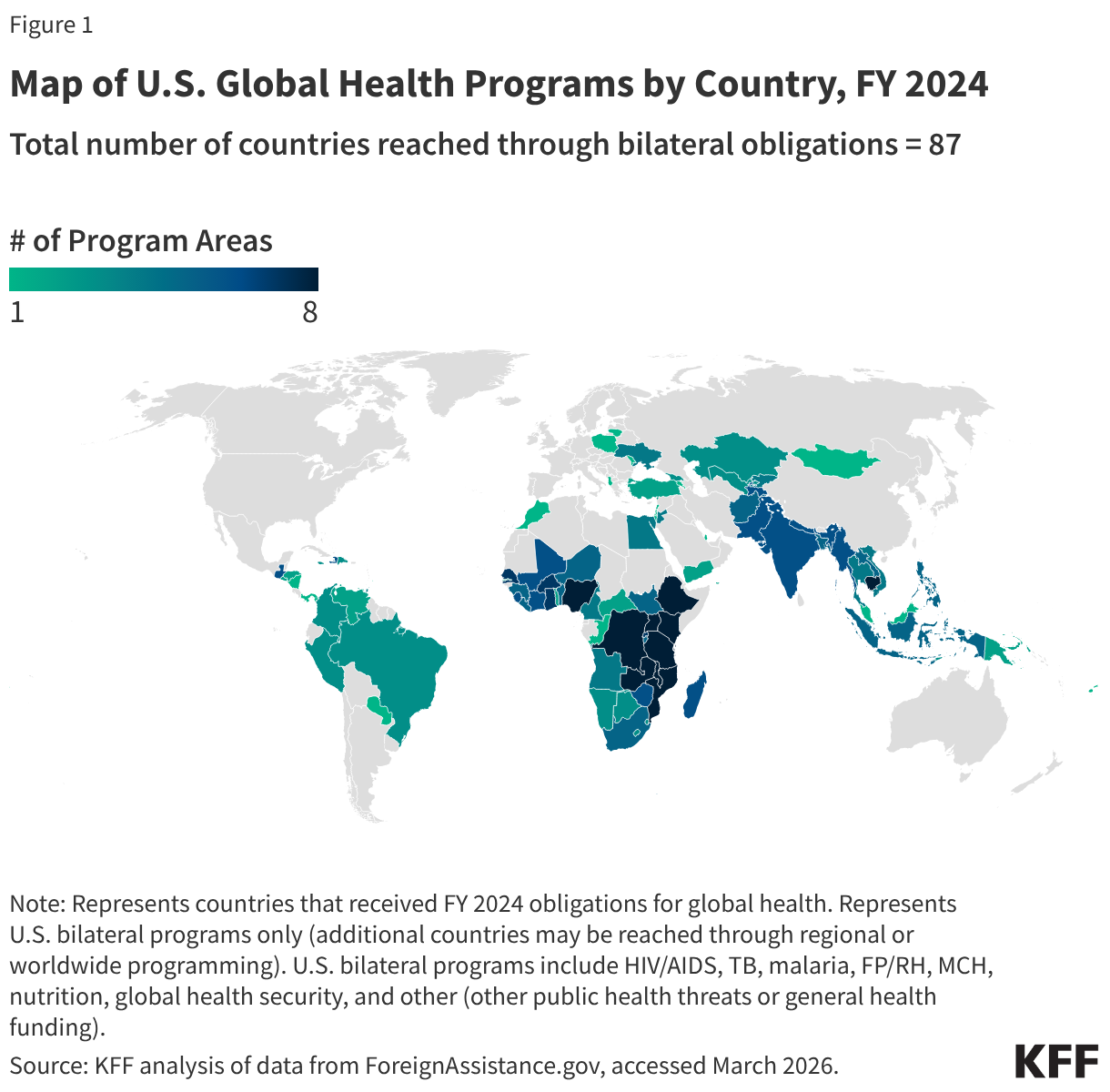
- Sub-Saharan Africa: Remains the primary recipient of bilateral aid, particularly through PEPFAR and PMI. Countries like South Africa, Nigeria, and Kenya host some of the most complex and well-funded U.S. health missions.
- South and Central Asia: Programs here often focus on TB control—with India being a major partner in the "End TB" strategy—and maternal health.
- Southeast Asia: The focus is heavily weighted toward Global Health Security and infectious disease surveillance to prevent the spillover of zoonotic diseases.
- Western Hemisphere: U.S. efforts in Latin America and the Caribbean often center on migration-related health needs, reproductive health, and vector-borne diseases like Zika and Dengue.
Official Responses and Policy Perspectives
Administration officials have consistently framed global health as a matter of national security. In a recent briefing regarding the FY 2024 budget, U.S. Secretary of State Antony Blinken emphasized that "health security is national security," noting that infectious diseases do not respect borders. USAID Administrator Samantha Power has also championed the "Localization" agenda, stating that for global health programs to be truly effective, they must be led by the communities they serve.
However, the program faces legislative hurdles. Congressional debates over the reauthorization of PEPFAR have highlighted ideological shifts regarding reproductive health and funding levels. Despite these debates, there remains a strong bipartisan consensus on the value of programs like PMI and TB control, which are seen as highly cost-effective interventions that enhance the U.S. image abroad.
Broader Impact and Economic Implications
The impact of U.S. global health programs extends far beyond the clinic walls. By reducing the burden of disease, these investments contribute to regional stability and economic growth. A healthy workforce is a more productive one; for instance, every dollar invested in immunization is estimated to return up to $52 in broader economic benefits.
Furthermore, U.S. global health assistance serves as a vital tool of "soft power." By providing life-saving medications and technical expertise, the U.S. builds long-term diplomatic relationships and fosters goodwill. In many partner nations, U.S. health programs are the most visible and positively perceived aspect of American foreign policy.
Challenges and Future Outlook
Looking ahead, the U.S. global health strategy faces several headwinds. The increasing frequency of climate-related disasters is disrupting health delivery systems and shifting the range of infectious diseases. Additionally, the rise of antimicrobial resistance (AMR) threatens to undo decades of progress in treating TB and other bacterial infections.

The FY 2024 data provided by trackers like those from the Kaiser Family Foundation (KFF) will be instrumental for policymakers to identify gaps in coverage. As the U.S. continues to refine its bilateral strategy, the focus will likely shift toward "health systems resilience"—ensuring that countries can maintain essential health services even in the face of future pandemics or environmental crises.
In conclusion, the U.S. commitment to global health in FY 2024 remains a cornerstone of its international engagement. By supporting programs in over 80 countries, the U.S. is not only addressing the immediate health needs of millions but is also building a more secure and prosperous global community. The data-driven approach of the current tracker ensures transparency and allows for the strategic recalibration of resources to where they are most needed in an ever-changing global landscape.



{kind=link}